LOADSAMONEY!
According to the sales pitch on Thursday from investment banks Credit Suisse and Morgan Stanley, a COVID-19 vaccine could be a “bumper revenue opportunity“, projected to earn at least $10 billion a year. Morgan Stanley’s projection is at least $10 billion a year across developed countries but Credit Suisse is bigging it up further still with a projection of $10 billion just from North America.
Financial projections by financial analysts in financial organisations that stand to gain financially. Can you spot the relevant word in that sentence (and no, it’s not ‘projections’ although that is a pretty close second)? These are companies with conflicted interests – and if they own any stock in any pharmaceutical companies, vested interests – in the development of treatments.
It is no surprise that their projections are per year because if you are going to monetise a vaccine as much as possible, you had better suggest that it is an annual vaccination. A vaccine administered annually…that’s not a vaccine, that’s an antiviral. Big difference.
Vaccine vs Antiviral.
A vaccine in general and a pandemic vaccine in particular is only effective against a specific pathogen that has very low mutagenesis, else the differences between primary infection (administering of vaccine) and secondary infection (subsequent infection with wild-type virus) will render the vaccine ineffective. The high level of recombination around SARS-CoV-2’s spike glycoprotein, notably its dynamic glycan shielding, as well as role of nonstructural protein nsp16 in immunoevasion suggest that a pandemic vaccine is unattainable.
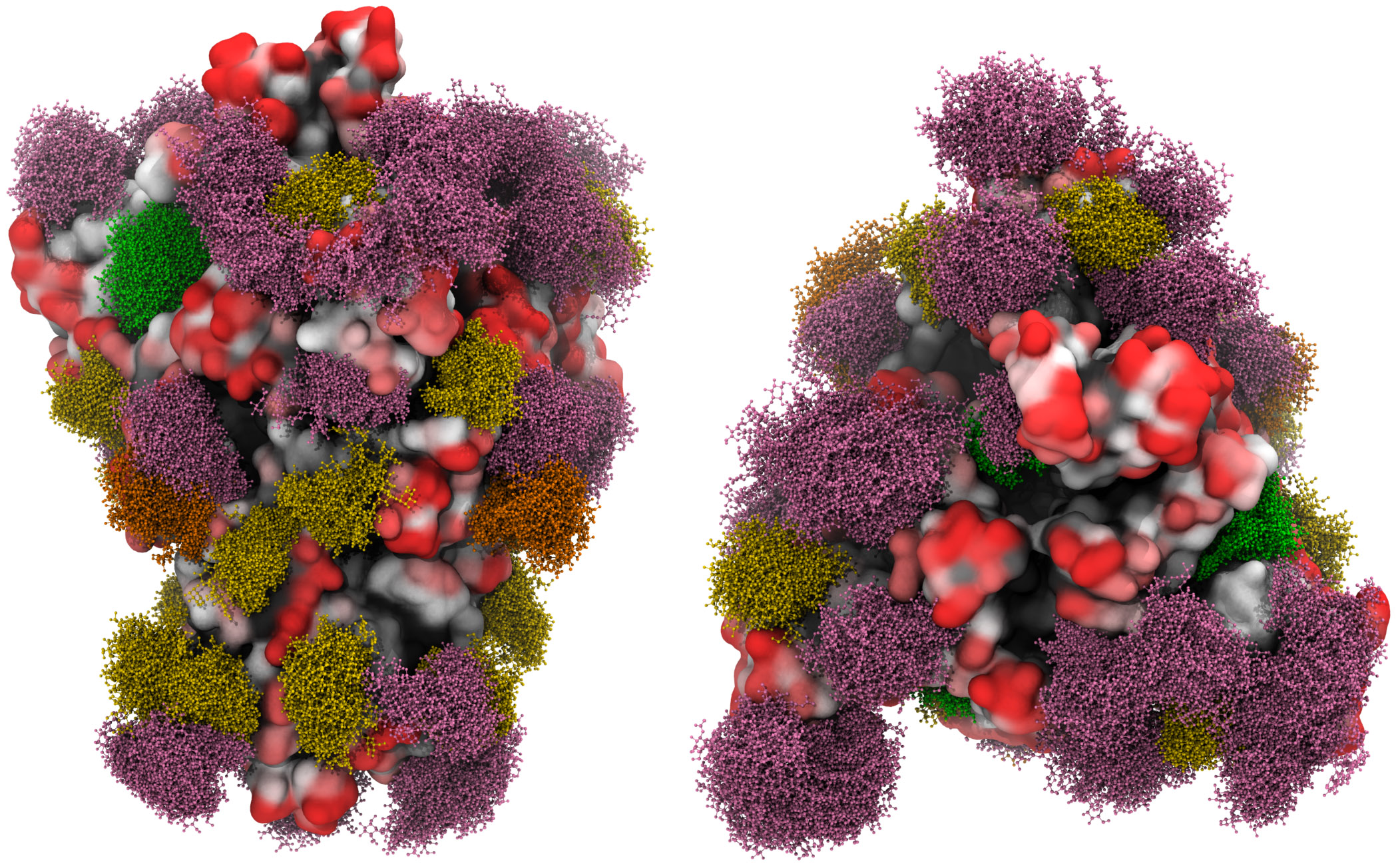
A three-dimensional molecular simulation of the spike glycoprotein with the moss effect showing the glycan shielding [Grant et al, 2020].
If a ‘vaccine’ has to be taken annually then it fails to support the fundamental function of the adaptive immune system: immunological memory. To understand why immunological memory is so important, you can read our previous explanation here.
A vaccine is unnecessary and unlikely to work but big pharma isn’t interested in a virus that is very effectively dealt with in the vast majority of people who get it by the innate immune system only, without bothering the adaptive immune system and therefore essential component for any vaccine to be effective. There is no money in that.
Bod and Bod…SNAP!
Fundamental to the innate immune response are leukocytes that carry pattern recognition receptors (PRRs) that are programmed to recognise pathogen-associated molecular patterns (PAMPs). Each pathogen has its own PAMP and this allows the immune system to identify a wide range of infections through PRR detection of their known molecular structure. PRRs thereby provide the body with the capability to deal immediately & automatically with a wide range of common infections without immunological memory and the creation of antibodies.
Given how long alpha and beta genus coronaviruses have been around – coupled with the fact that four of them cause the common cold – it is logical to deduce that a newly-discovered beta genus coronavirus contains a PAMP that can be detected by PRRs given they recognise existing alpha and beta genera coronavirus RNA This is particularly relevant if SARS-CoV-2 gained its furin cleavage site through recombination with CoV-OC43.
Nothing to see here from a monetising opportunity, sorry.
Why There Are No Existing Coronavirus Vaccines.
There are currently no vaccines for the pathogens of the coronaviridae family which sounds scary until you understand this is because most are not pathogenic to humans and most of those that are pathogenic are dealt with effectively by the innate immune system. No vaccine required.
Following SARS-CoV in 2002 and MERS-CoV in 2012 (both betacoronaviruses), developmental work was undertaken but has not progressed beyond phase I clinical trials [Modjarrad et al, 2019]. The reasons for this include the localised nature of the SARS-CoV and MERS-CoV outbreaks, the lack of source material and fact that SARS-CoV ceased to be reported after 2004, so there was no need – medical, financial or otherwise – to develop a vaccine.
The fact that there is now a newly-discovered betacoronavirus (remember, it isn’t ‘new’ simply because you only discovered its existence earlier this year) means that the question of a vaccine comes to the fore again, especially when the woeful handling of the situation by governments dictates a vaccine has to be invented in order to justify the hysterical threat posed by the killer virus of death (that keeps on not killing people, especially those it infects). Unlike, say, a flood or hurricane, a virus does not cause the closure of businesses, loss of jobs or ruin of an economy. That is down to the government response.
Passive Immunity Through An Antiviral.
We have posited previously that the best outcome is likely to be an antiviral that can be expected to be 50% effective at best and which may provide passive immunity to those with weakened immune system. These are the people lacking immunological memory, for whom a vaccine isn’t going to work so a therapeutic antiviral may help.
As an antiviral, the most obvious comparison is with the seasonal or winter flu antivirals oseltamivir and zanamivir. We have recently analysed their efficacy – or more precisely the lack of it – and subsequently looked at the results of further clinical studies. These maintain the conclusion that seasonal or winter flu antivirals have minor benefits to those in high risk groups (benefits that may well not outweigh the adverse side effects) and no noticeable impact on reducing hospital admissions. In terms of ‘stopping the spread’ of seasonal or winter flu, you would need to give antivirals to 71 people to prevent just 1 case of flu [Cochrane, 2016].
Think about that for a minute or two or 71. Just how much more effective is a COVID-19 antiviral going to be? For our detailed analysis of why remdesivir is not an effective antiviral for COVID-19 read here.
Of course nobody wants to hear that at the moment, as big pharma falls over itself in the gold rush to roll out a vaccine/antiviral at the earliest opportunity, dispensing with the usual time scales and checks & balances necessary to show that what is being pumped out is safe and effective. Wow that mouse just exploded…better put that test result down to indigestion.
Smaller Than The Flu.
The sheer pointlessness of a vaccine can be deduced from Stephen Hoge, CEO of Moderna, the American biotech company developing a potential vaccine mRNA-1273, who said; “it’s a smaller opportunity [than flu]. It’s not a trivial one.” As an aside, a messengerRNA vaccine…hmmm, a kind of experimental vaccine that has yet to be approved anywhere in the world for any illness, as set out in our earlier article.
If you defer to the core principle of stimulus & response, if the response is being touted as something taken annually just like a flu shot and likely by smaller numbers, then the stimulus has to be no more dangerous than flu. As we have been saying since early March.
But ‘Oh no, you might be able to get ‘the coronavirus’ more than once!’ proclaim the media.
The more SARS-CoV-2 evolves, the faster it has to in effect run – hence an increase in the R0 ratio, which is dynamic during an infection’s life cycle – to avoid herd immunity, i.e. to find those who haven’t already had it and that ‘speed’ comes at the expense of virulence. In weakens, in effect becoming more like the common cold, mimicking fellow beta coronaviruses CoV-HKU1 and CoV-OC43.
If you can get it more than once, then it isn’t bothering the adaptive immune system as it is being dealt with by the innate immune system only. Just like the common cold. No vaccine required.