Infectiousness Or Infectivity.
If the government is to be believed, the new killer mutant of death (no, not vaccines minister Zoonotic Gaddafi, the other killer mutant of death known as N501Y) is even more infectious and even more transmissible. Except the government likes to confuse viral infectiousness with disease severity. They are very different. Also, it is important to understand the difference between infectiousness and infectivity. To clarify them, infectiousness is the capacity of a pathogen to infect others, i.e. to spread, whereas infectivity is the capacity of a pathogen to cause infection. Infectivity is related to severity but infectiousness is not. Our default example is varicella-zoster virus (chickenpox) that has an R0 ratio in the range 10 – 12 compared to ebolavirus that has an R0 ratio in the range 1.5 – 1.9. Chickenpox is way more infectious or transmissible but would you rather have chickenpox or ebola? So N501Y is more infectious but it is not more dangerous, unless you follow government advice or think the NHS is doing a good job.
Also known as B1.1.7 (SARS-CoV-2 being a sarbeco or lineage B beta genus coronavirus) or S-VoC (variant of concern), N501Y is the talk of the town as it may be ‘up to 70%’ more transmissible and could result in much higher levels of viral load. The first point to draw from this is it is variant of concern not mutant of concern or killer mutant of death. At least some sanity prevails somewhere.
Learn From The D614 To S614 Switch.
SARS-CoV-2 underwent a variation in early 2020, with an A→G single nucleotide polymorphism causing a change in one of the amino acids that form the structural spike protein. This altered the spike protein from SD614 to SG614 and made SARS-CoV-2 more infectious. It did so by reducing S1 subunit shedding. As we explained back in September the trimeric spike glycoprotein has two subunits: S1 that binds the virion to the receptor binding domain and S2 that effects cellular membrane fusion & cellular entry. By reducing S1 shedding [Zhang et al, 2020], it increased the expression of S1 thereby allowing it to bind to more receptors, which makes it more infectious. However SG14 does not bind more effectively or cause any increase in infectivity/disease severity [Zhang et al, 2020; Korber et al, 2020; Groves et al 2020]. Within three months, SARS-CoV-2-SG614 took over from SARS-CoV-2-SD614 and became the dominant, near exclusive variant globally:
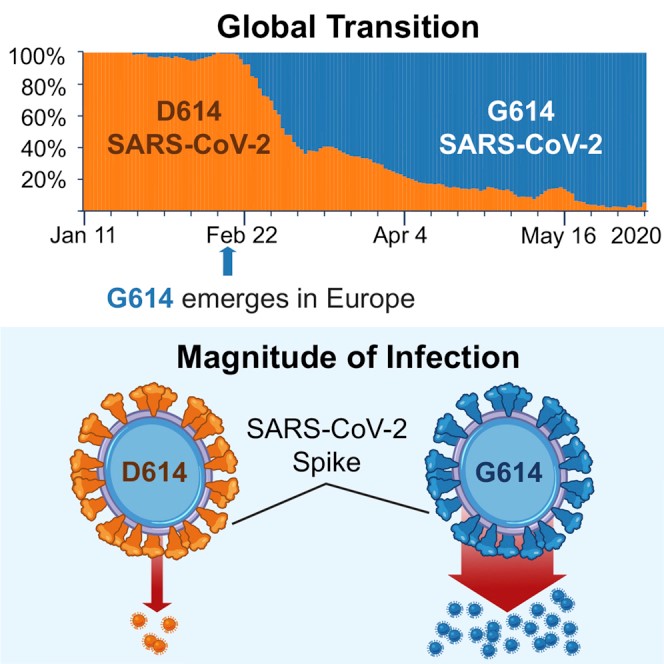
Emergence of variant SG614, [Korber et al, 2020].
In simple terms, SG614 is fitter. It can run faster and therefore infect more people [Korber et al, 2020]. It is fitter because viruses apply natural selection as part of their survival mechanism. It is however no more dangerous in itself unless you ignore viral load.
SG14 causes higher viral load concentrated in the upper respiratory tract and as S-VoC / N501Y can increase viral load, the upper respiratory tract is the key area in which to target viral countermeasures. Which highlights the fallacy of all the IM/ID delivery ‘vaccines’ that target IgG isotype and bypass the upper respiratory tract, secretory IgA and do not provide sterilising immunity [Krammer et al, 2020; Dolemaren et al, 2020; Yu et al, 2020].
Viral Load Is Even More Important.
The relationship between – and crucial importance of – viral dosage and viral load is something we first highlighted back in April and have been banging on about pretty much ever since. We have been focusing upon this particular issue for nine months now because understanding viral dosage & viral load is what saves and not understanding it is what, sadly, costs lives. It is the reason the government strategy and government & NHS response are responsible for the majority of UK deaths, as lockdown increases viral load and NHS deathfactories and staff were the reservoirs for the highest levels of viral load in the land.
If you leave SARS-CoV-2 alone and treat it like a seasonal irritant, which is exactly what it is, nothing more nothing less, then you don’t have a problem. Yes, be aware of those in high risk groups (those with relevant comorbidities and those with renin-angiotensin system issues and dysfunction to the ACE2→ Angiotensin1-7→ Mas / ACE→ angiotensin II→ AT1 receptor axes) but for everyone else, let them carry on as normal. It is precisely because the government locked people away that so many have died. The reason so many in care homes have died is because residential and nursing care environments are akin to lockdown anyway, i.e. individuals confined in the same place for sustained periods of time and in close proximity to the same individuals.
Lockdown Increases Cases Of N501Y / S-VoC.
Movement, getting outside and gaining persistent antigen exposure from different individuals really do make people safer when it comes to SARS-CoV-2. Lockdown and social distancing really do make the situation worse. This is proven by Volz et al. who identify that “it is clear that while lockdown successfully controlled S+ cases…S-case numbers increased during lockdown.” S- cases relate to the Sgene target failure variant, aka Sgene dropout, aka B1.1.7, aka N501Y, aka S-VoC.
It is worth highlighting that this variant is designated ‘failure’ or ‘dropout’ because it tends to not show up in RT-PCR testing. Ha! This is a result of the deletion of amino acids H69 & V70 from the spike protein. ΔH69/V70 deletion is frequent in SARS-CoV-2 [Kemp et al., 2020] and represents antigen shift through the dynamic glycosylation around the spike protein. If nucleic acid wasn’t already discredited enough for being hopelessly flawed, incorrect as any measure upon which to make any sensible decision, prone to more false positives & false negatives than correct results and prone to detect the common cold (as a lineage A beta genus coronavirus), it certainly is now. Kidd et al. identify S-VoC as having a 27.7% dropout rate in RT-PCR testing, leading to their comment that it can “show a suboptimal profile in RT-QPCR tests“. That’s an understatement, especially when Kidd et al.’s study was funded by the Department of Health and Social Care.
We are now going through a similar variation with N501Y. It is fitter than its fellow variants so it will likely become more dominant, applying the same principle of natural selection. However, once again, its greater rate of infection or transmission is NOT linked to increased disease severity. The WHO’s own conclusion is that N501Y has “no change in disease severity—as per hospitalization length and 28-day case fatality—nor reinfection risk.”.
N501Y / S-VoC Is Not More Dangerous Unless You Follow Government Advice.
S-VoC is more transmissible but so was SG614 and likewise S-VoC is no more dangerous than SG614 [Korber et al, 2020] unless you ignore the relevance of viral load. Volz et al. have proven that lockdown plays into S-VoC’s hands, as it provides the ideal environment in which to allow viral load to accumulate to levels where the innate immune system is unable to overcome it. So the latest lockdown is literally a death sentence passed on anyone foolish enough to believe the worthless inventive and misinformed lies spouted by ignorant politicians and conflicted public health professionals. Career civil servants who have never taken a risk so they don’t understand risk. Career civil servants who are so afraid of covering their backsides and preserving their grotesque pension they will send tens of thousands to their deaths rather than simply say ‘sorry, I was wrong’ and stop this genocide.
We have explained both antigen shift and drift in several previous articles and S-VoC / N501Y is nothing more than one or both of these factors at work around the spike protein as part of SARS-CoV-2’s phylogenetic evolution through natural selection. Both alpha genus and lineage A beta genus cold-causing coronaviruses do it [Chibo and Birch, 2006; Ren et al., 2015; Vijgen et al., 2005] and lineage B beta genus coronaviruses are no different [Guan et al., 2003; Song et al., 2005].
What is noteworthy is that a single nucleotide switch – D480A→G – resulting in an amino acid change within the spike protein of SARS-CoV meant that it evaded antigen-specific nAb 80R. Genetically-modified chimpanzee-virus vaccine ChAdOx1 assumes a static spike protein without any antigen shift or drift. Quite apart from it being IM delivery and therefore unable to stimulate secretory IgA and provide protective or sterilising immunity (i.e. you can still catch and spread SARS-CoV-2 even if ‘vaccinated’) ChAdOx1 may already have been rendered obsolete by S-VoC.
Do not allow yourself to be misled by the fearfest of government lies and NHS propaganda. As with SG614 before it, S-VoC / N501Y is more infectious but no more dangerous. Unless you follow government advice.