What Is Nucleic Acid Testing?
Nucleic acid testing, more commonly known as PCR or RT-PCR testing, is one of the three main types of viral testing. There is a full explanation of these three types here but concentrating on PCR testing, it tests a sample for tiny fragments of viral RNA. It shows only the presence of those fragments and cannot differentiate between live RNA (in virion or infected host cell) and dead RNA (in viral debris). Neither can it identify when, where or how the RNA got there. It is purely an indication of the presence of viral RNA. PCR testing takes the sample and goes over it time & time again (cycling) to try and detect a result and then assumes (amplification) that what it detects is the target substance, in this case SARS-CoV-2.
You Do The Math.
Coronaviruses have some of the longest genomes of all RNA viruses, with SARS-CoV-2 having 28,936 nucleotides. Three nucleotides form a codon that forms an amino acid. A single amino acid change, caused by insertion, switch or deletion of a single nucleotide, can render a virus invisible to PCR test if that particular amino acid was one of the target fragments. As we explained last week, S-VoC – aka N501Y, aka Sgene dropout, aka Sgene target failure – often doesn’t show up in PCR testing. Kidd et all show a 27.7% dropout rate (hence the latter two designations).
Antigen shift through glycan shielding around the S protein is SARS-CoV-2’s dynamic natural defence and S-VoC is a direct result of this through the ΔH69/V70 amino acid deletions in the S protein.
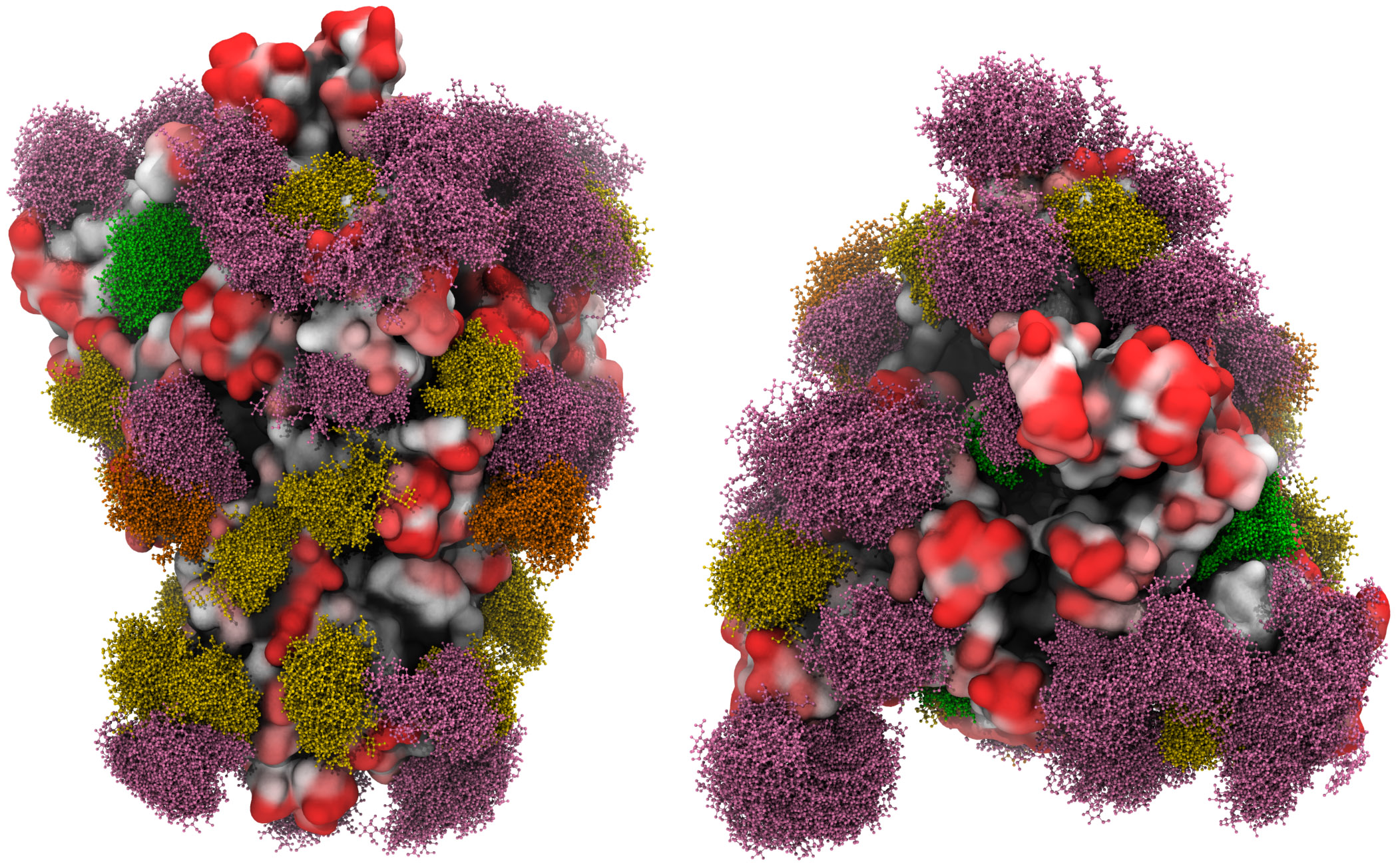
A three-dimensional molecular simulation of the spike glycoprotein with the moss effect showing the glycan shielding [Grant et al, 2020].
A minimum two & maximum six nucleotides are required to cause two amino acid changes. Two to six out of 28,936…good luck with using PCR testing as any measure of accuracy or – worse still – any basis upon which to make any decision.
That’s before you factor in the margins for error, with some nucleic acid tests returning up to 30% false negative and 30% false positive. As well as the homology of coronavirus genetic sequences, meaning PCR testing can’t tell the difference between lineage A and lineage B beta genus coronaviruses, i.e. between a common cold and SARS-CoV-2. Spot the difference:
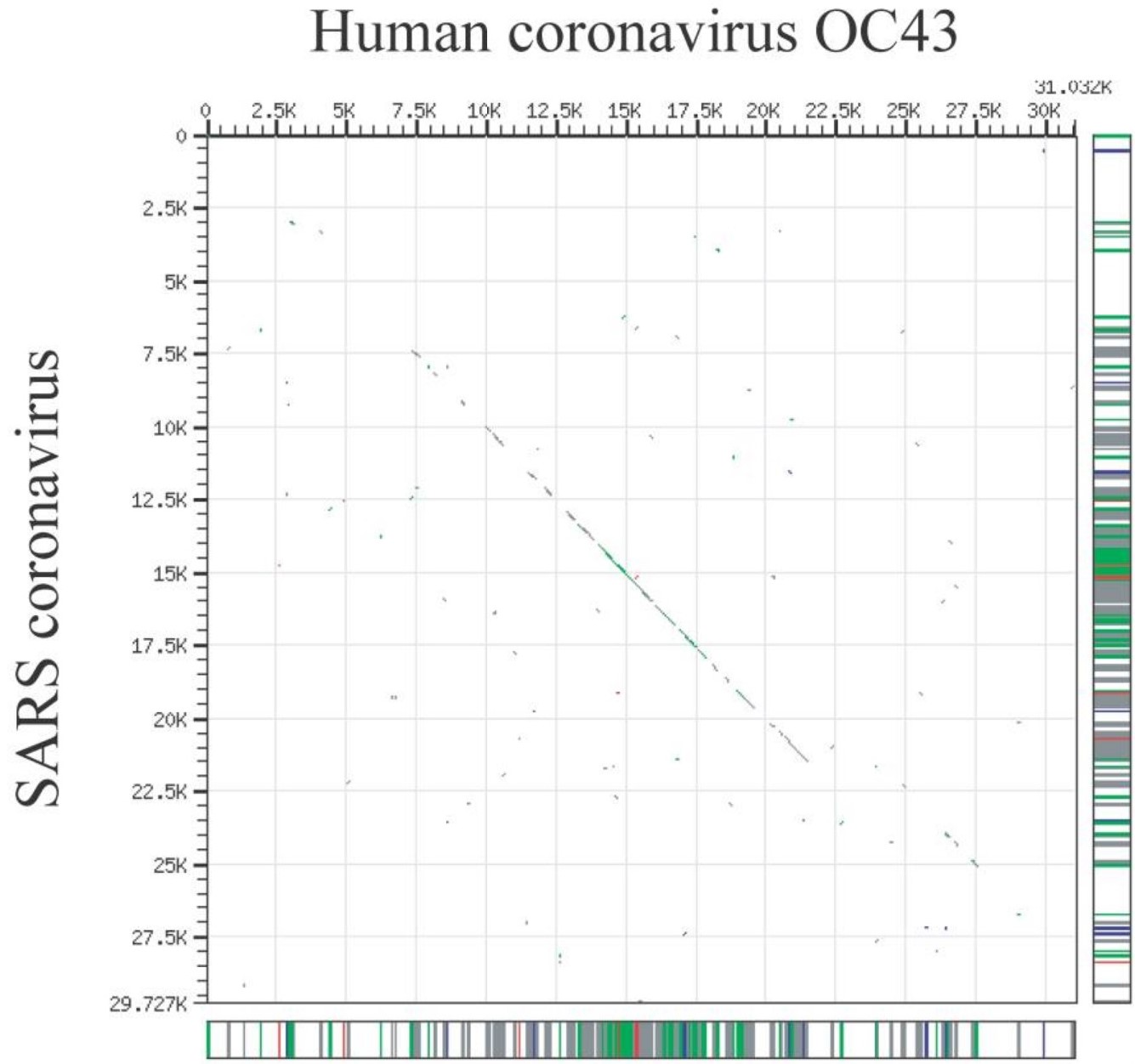
Maizel-Lenk dot plot showing the homology of HCoV-OC43’s genetic sequence with that of SARS-CoV, [Vijgen et al, 2005].
Our research is currently focused upon SARS-CoV-2 having started to attenuate around May 2020, as a result of the amino acid changes that caused the SD614 to SG614 switch, something that we explain here. We will set out our findings more fully in due course but the data supports the view that by August SARS-CoV-2 was weakening and it has continued to attenuate since then, as we set out on 31st August; 30 November; 5th January and most recently five days ago.
What The WHO Has To Say.
So, the starting point is that nucleic acid testing is inaccurate, prone to huge levels of error and doesn’t really tell you anything. Yesterday, the WHO issued an update for users of In Vitro Diagnostic Medical Devices (IVD), advising them – in simple terms – to ‘check their equipment’ and therefore by implication for anyone looking at the results produced by that equipment to ‘check their results’. This is because the equipment is prone to chuck out incorrect data and here is why, in the WHO’s own words:
“The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load”…”disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases“.
And if that were not enough, which for any rational individual it should be, they go on to say;
“This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
In other words, as an infection’s life cycle progresses, more people have had it and the infection itself attenuates, PCR testing becomes more inaccurate and likely to show more false positives.
The WHO concludes that PCR tests “are indicated as an aid for diagnosis” and myriad other factors should be taken into account when considering a test result. One of these is “confirmed status of any contacts” which is completely different to the random, haphazard and ineffective nature of the UK’s track and trace debacle. One has to question whether the £22 billion cost will save a single life. One can only imagine what £22 billion could have bought in terms of social care and medical resources..
Just in time then for the forced testing of schoolchildren. As an aside, as it is forced because if a parent declines – as is their right as they are responsible for their child’s safety – they are not allowed to send their child to school, does that make it a form of child abuse? Having spent years falling over themselves educating everyone on the dangers of bullying and too much screen time, it now appears education is conducted by endless hours of daily screen time. Plus any child who has a high temperature (hint: it’s pyrexia and perfectly normal, as we set out here) or delivers a positive PCR test (which of course will more than likely be a false positive) is now systematically bullied by the rest of their academic year.
If you bullied your child; forced them to perform acts they didn’t want; left them home alone for hours on end and made them stare at a screen for hours every day, social services would be around your house like a shot. Except untrained, unchecked but apparently adequately supervised strangers can now test your child in a manner that would have any individual with a competency in safeguarding having a fit. Let alone the stigma and inevitable bullying that then accompany any child who tests positive. There are myriad instances of kids who have falsely tested positive for SARS-CoV-2 – when the pyrexia was caused by an ear infection – being called ‘AIDS boy’, ‘Jew!’ or ‘virus girl’, compounded when they are from an ethnic minority.
What Is PCR Testing Actually Good For?
As a basic analogue, it can indicate that something has happened. As an example, an outbreak of food poisoning in cheese is caused by listeria monocytogenes. The cheese was manufactured in a single location but sold nationwide through a chain of shops. Nucleic testing of individuals presenting with symptoms of food poisoning who live close to the location of the shops would give you an indication of the level of infection. The data might help direct relevant resources to deal with the illness. However, PCR testing is backward looking as it tells you something has happened but not when it happened or whether the pathogen being tested for is live or dead (having already been overcome by the body’s immune response).
As a tool for use in the response to SARS-CoV-2, nucleic acid testing is pretty much useless. We first highlighted this in March 2020, explored its fallacy further in September and again in December. Now, it seems that 10 months after we raised our concern, the WHO agrees.