UK Deaths Increase By More Than One Third Since Vaccine Rollout.
In the four weeks since the ‘vaccine’ rollout, UK COVID-19 deaths have risen by 31,368 (source: Johns Hopkins Coronavirus Resource Center and Worldmeters, @0500UTC 18/02/21). As the ‘vaccine’ is being offered to those in high risk groups first, it does not follow that over the four weeks since the start of its delivery, UK total deaths have increased by 36.2%.
An increase of just over one third in one month should be an enormous red flag. Especially when daily deaths across the rest of the world have fallen significantly over the same period:
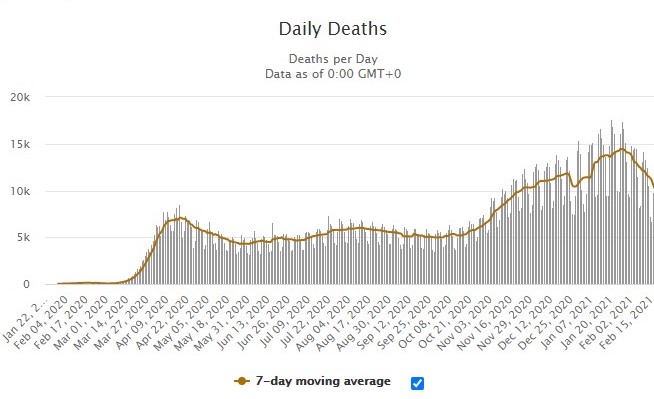
If the increase in total deaths were not bad enough, the UK continues to occupy a top five position in the highest mortality rates on a worldwide basis. This comparison maps COVID-19 daily deaths globally against the UK for two days ago (Wednesday 17th February):
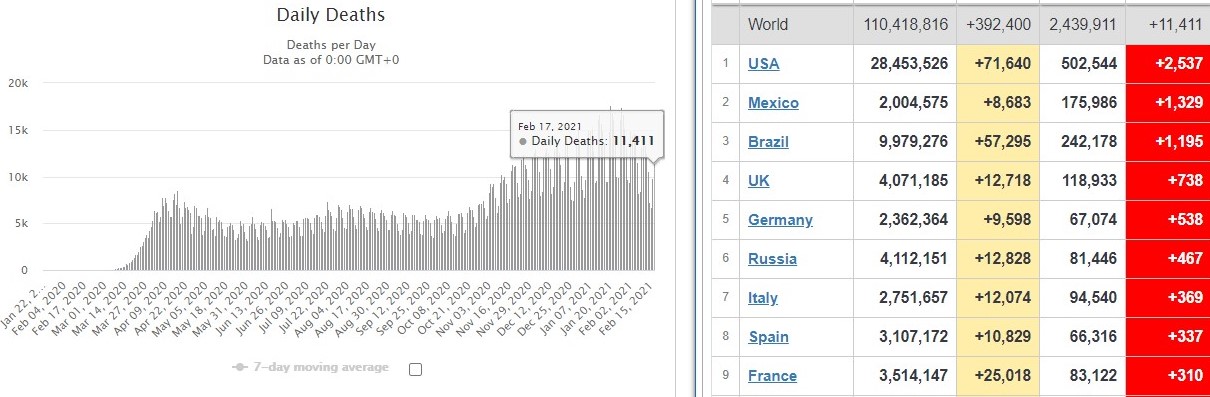
Of the 11,411 daily deaths across the entire world, 738 of them were in the UK. That’s 6.47% of the total daily deaths from a nation that accounts for 0.87% of worldwide population. Again, this should be a red flag.
Likely Reasons.
- As we first highlighted in October 2020, there is a fundamental difference between a vaccine and an antiviral. For some reason, the UK government and healthcare leaders misleading refer to ChAdOx1 and BNT126b2 as vaccines when they are antivirals.
An antiviral is a drug given to someone either when they are infected with a virus or immediately preceding likely infection. For example, some antivirals for influenza A serotypes must be taken within two days of infection to be effective. The sole function of an antiviral is to attenuate or reduce the pathogen’s infectivity for the here & now. Antivirals are therapeutic in nature, working only for a short period of time and in effect are a one-time treatment to make you feel less ill. A vaccine is a drug given to someone before they are infected with a virus. The function of a vaccine is to give an individual long-term – ideally permanent – protection from the virus and in general vaccines are prophylactic in nature, creating active immunity for the future.
These ‘vaccines’ are not miracle cures or wonderdrugs. At best, they are antivirals designed to attenuate disease severity in those with COVID-19 symptoms and/or reduce recovery time. They do not stop an individual from catching SARS-CoV-2 or from spreading it. With UK deaths having risen by one third in the four weeks since rollout, the data suggests that they are not even very effective antivirals.
- Even worse than an antiviral – or vaccine – being ineffective is where it makes the situation worse, causing the immune system to malfunction and mistake ‘self’ for ‘non-self’ (self/non-self is arguably the most fundamental function of the immune system) triggering autoimmunity and immunopathology. In addition, there is the potential of antibody-dependent enhancement (ADE) and antibody-dependent cell-mediated cytotoxicity (ADCC).
ADE in particular is a proven risk in coronaviruses in general and contributor to disease severity in sarbecovirus / lineage B betacoronaviruses SARS-CoV [Ho et al, 2005; Bolles et al, 2011; Tseng et al, 2012] and SARS-CoV-2 [Zhao et al, 2019; Gao et al, 2020; Chao et al, 2020]. This is why true vaccines take 10-15 years to develop, rather than less than one year.
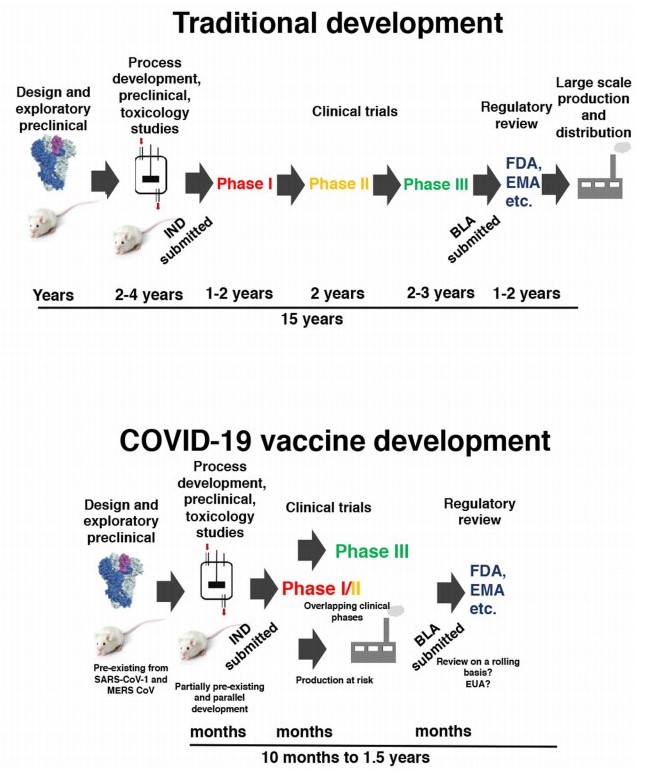
Timeline for standard and rushed COVID-19 vaccine development [Krammer et al, 2020].
- During the final stages of the viral replication process, not all newly-replicated structural spike proteins are transported from endoplasmic reticulum to endoplasmic reticulum–Golgi intermediate compartment (ERGIC) for assembly of the virion in preparation for exocytosis. Instead they travel to the host cell membrane and effect cell-to-cell fusion, binding to adjacent cells. This process creates clusters of cells with multiple organelles, allowing increased replication without detection by antibodies. In effect, it is a clever Plan B that provides a higher degree of immunoevasion, as these S proteins are invisible to vaccines or antivirals that aim to stimulate IgG isotype antibodies programmed to recognise the S protein’s epitopes.
- As these antivirals are intramuscular or intradermal delivery they bypass the upper respiratory tract. We first identified the crucial importance of viral load in April 2020 in respect of its positive correlation with disease severity. A more expansive evaluation of the upper respiratory tract in preventing infection and transmission is set out here. Viral load is why you do not confine people in close proximity to others for sustained periods of time, which of course is exactly what the UK government did and this is one of the main reasons for the UK mortality rate has always been several times the worldwide average.
Lockdown increases viral load that causes increased disease severity.
A Pause In The Rollout Is Essential To Save Lives.
An increase in total deaths of more than one third in four weeks since treatment rollout should be a massive red flag, when total daily deaths and mortality rates are falling across the rest of the world. Simultaneous to the mass roll-out of a treatment, this should be of enormous concern.
The government strategy and government & NHS clinical response are the reasons why the UK is one of the most dangerous places on the planet and they are now responsible for more than 97,930 deaths, up from 69,663 just one month ago.
SARS-CoV-2 is a seasonal irritant. It poses a danger to a very small group of people, around 0.4% of the population, in exactly the same way as does any respiratory virus and arguably any pathogen that can act as a causative agent for secondary infection. SARS-CoV-2 was never – and is not – the killer virus of death. Instead, it has been turned into one by government strategy and the government & NHS clinical response. It now appears that the miracle cure is nothing of the sort – it never was – and may well be making the situation even worse.
As a minimum, it would be prudent to pause the rollout and identify the root causes of the issue because for every day that you don’t, more people will die unnecessary and avoidable deaths. Except a pause would likely highlight the flawed nature of the treatment, so what are the odds that the government will continue blindly down the cul-de-sac of its ignorance?
Celebrating ‘vaccinating’ 15 million individuals does not justify killing 31,000 individuals to achieve it.
Do not panic. Do not worry. Do not follow government advice.