Just What Is Different About Delta?
B1.617.2/Delta is apparently still spreading. This is unsurprising given that it has been occurring globally for over eight months. At least the WHO has finally applied a nomenclature to the main SARS-CoV-2 variants, adding to the existing PANGO and Nextstrain designations. This validates something we first highlighted four months ago: it is incorrect to name variants geographically because haplotypes do not just spring up in one country. Unfortunately, this basic fact of viral phylogenesis continues to escape the understanding of the UK government, which likes to make out that we should all be afraid of the ‘Johnny Foreigner’ virus and impose a raft of pointless restrictions to try and stop people bringing something back with them that has been occurring in the UK and other countries all along. After all, it’s called Delta and there is the Delta Force and then there was that velociraptor in Jurassic Park, which was pretty scary.
The Delta variant if you are Boris Johnson or Chris Witty (hint: Jurassic Park was sciency fiction not science fact):

Image courtesy of the Jurassic World Alive Wiki.
As a result of deletions at amino acid positions 156 & 157 within the S1 subunit as well as a threonine to lysine substitution at 478, Delta is more infectious than B1.617.1/Kappa and B1.617.3, as is also B1.1.7/N501Y.v1/Alpha (formerly the ‘UK’ variant). Again this is unsurprising, this time for two reasons:
- 478 and 484 are around the receptor binding domain (RBD) motif and a lysine substitution here increases recognition of and therefore binding affinity to the ACE2 receptor on target cells. Shang et al., [2020] show that 493 is the likely position that first enabled SARS-CoV-2 to become pathogenic. This is why there is a lysine substitution at 484 that is present in Beta (B1.351/N501Y.v2, formerly the ‘South African’ variant), Gamma (B1.1.28/P1, formerly the ‘Brazilian’ variant) and intermittently within Alpha. Delta simply applies the same substitution a few positions earlier within the RBD.
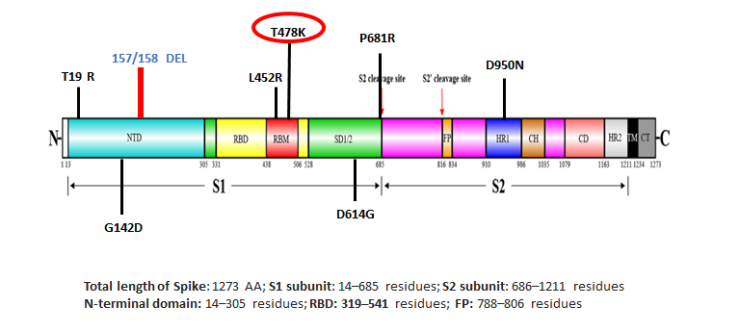
Delta/B1.617.2 variant structural spike protein domain. Source: https://science.thewire.in.
- Alpha also has similar deletions (at 69, 70 & 144) and this type of indel is designed to create a fitness advantage, i.e. more infectious = greater chance of survival. However, 𝗶𝗻𝗳𝗲𝗰𝘁𝗶𝗼𝘂𝘀𝗻𝗲𝘀𝘀 𝗶𝘀 𝗻𝗼𝘁 𝘁𝗵𝗲 𝘀𝗮𝗺𝗲 𝗮𝘀 𝗶𝗻𝗳𝗲𝗰𝘁𝗶𝘃𝗶𝘁𝘆.
Infectiousness vs Infectivity.
There is a fundamental difference between these two key terms, as we explained in January, yet the UK government continues to deliberately confuse the two words, in order to make something with greater infectiousness but not infectivity sound like it has greater infectivity. Delta has no greater infectivity than Alpha, Beta, Gamma or B1.617.3.
In yet another irony of epic proportions, both Alpha and Delta are more infectious in household environments [Kidd 𝘦𝘵 𝘢𝘭., 2020; Allen and Vusirikala 𝘦𝘵 𝘢𝘭.], i.e. when you confine the same people together in close proximity to each other for sustained periods of time. Lockdown increases both Delta and Alpha’s infectiousness.
501 and 484 are two of the main positions for amino acid substitution with both having been occurring around the world for over fifteen months now. These substitutions occur naturally as part of SARS-CoV-2’s phylogenetic evolution. They are always going to be detected somewhere first but that does not mean they originated there and certainly does not mean they are exclusive to one geography.
Greater Escape Neutralisation From ‘Vaccines’.
Kappa poses a lower risk than Alpha because it substitutes glutamine not lysine at 484 and arginine not histidine at 681. These are neutralisation escape variations, as part of SARS-CoV-2’s ‘adaptive camouflage’ or ‘stealth mode’. Neither glutamine nor lysine substitutions are present at 484 in Delta but it has distinct variations in its genetic sequence, as set out above, meaning it is better at escaping neutralisation by antiviral-induced antibodies, i.e. the antivirals (they are not vaccines) are even less effective against Delta than they are against the other main variants. Our evaluation of Garcia-Beltran et al.’s study shows just how ineffective BNT126b2 and mRNA-1273 are against Alpha, Beta and Gamma. Why? – Quite simply because they target epitopes on the S protein, which is subject to antigen shift, i.e. adaptive camouflage or stealth mode.
Delta’s haplotype is designed to provide greater escape from vaccine-induced antibodies, as evidenced by reduced neutralisation in post-vaccination sera. The circulating vaccine-induced antibodies are more likely not to recognise Delta as well as most other variants because they are – in simple terms – using an ‘old photo’ or obsolete version. Conversely, your adaptive immune system responds to all SARS-CoV-2 variants as it encounters them. Through the lymphocyte receptor repertoire and somatic recombination, the immune system generates a unique response to whatever variant it detects. In simple terms, it always uses a ‘new photo’ or the latest version.
This is one of the many reasons why you do not target an adaptive S protein domain with an antiviral that requires it is to be static. We have been vehement critics of targeting the S protein domain, as we set out in February, with our position validated further by the WHO’s pronouncement that even those ‘vaccinated’ should continue to wear a non-surgical face covering to keep themselves ‘safe’ from Delta. If you have been ‘vaccinated’ but are still at risk of Delta then the ‘vaccine’ does not work. Or was never required in the first place.
Furthermore, it proves the total fallacies of ‘vaccinating’ healthy people; targeting the spike protein of a virus with a highly dynamic structural spike domain; focusing upon IgG rather than IgA antibodies and ignoring those elements of the innate immune response that kill SARS-CoV-2 virions within minutes of detection.
Conclusions.
- Delta is more infectious than Gamma and Kappa but less infectious than Alpha and Beta. Remember that Alpha has been endemic in the UK since Autumn 2020.
- Delta does not have greater infectivity compared to Alpha, Beta, Kappa and Gamma.
- Delta shows greater immunoevasion through escaping neutralisation by antiviral-induced antibodies, as shown in post-vaccination sera.
- Delta has been occurring globally for over eight months as part of SARS-CoV-2’s natural selection through fitness advantage and immunoevasion. In this respect, Delta is distinct to Kappa and B1.617.3 in that they show greater immunoevasion only.
The claimed ‘spread of the Delta variant’ is misleading at best and should not form the basis for any decisions. Delta is another variant that proves though escaping neutralisation that the antivirals being injected into individuals are ineffective. Rather than be honest with people and admit this, the UK government continues to deliberately confuse ‘infectivity’ with ‘infectiousness’ with the aim of making out that greater infectiousness = greater infectivity. It does not.