The Poorer The Country, The Lower The Mortality Rate.
This is the first pandemic in history where ‘poorer’ countries fare better, usually far better, then ‘richer’ ones. The more developed the country; industrialised the economy; advanced the healthcare system; widespread the adoption of Western lifestyle & diet, the higher the total deaths and in most instances the mortality rate. We first highlighted this back in January, illustrating just how badly the UK had fared in terms of its COVID-19 mortality rate.
Currently, nine of the ten countries with the highest COVID-19 total deaths are G20 countries. G20 nations make up 15 of the 20 highest COVID-19 total deaths. North & South America account for 48.4% of all COVID-19 deaths globally. (Source: Johns Hopkins Coronavirus Resource Center/Worldmeters, @ 0500UTC 14/07/21.) This is not a coincidence.
For SARS-CoV-2 think ‘lifestyle virus’ and for COVID-19 think ‘Western diet disease’.
The link between Western diet and multimorbidities is well-proven but with COVID-19, there is evidence that Western diet trains the innate immune system the wrong way. Excess cholesterol introduces a bias into myelopoiesis, in both leukocytes and their progenitor haematopoietic stem cells. This then causes increased sensitivity to infection and then over-expression of cytokines. Cytokine storm is one of the two main causes of death linked to COVID-19 and is mediated if a ‘trigger happy’ innate immune system stimulates an excessive inflammatory response.
Vitamin D Deficiency.
It is ironic that coronaviruses are named after the sun when sunlight is their kryptonite. The vitamin D pathways provide both immunity from SARS-CoV-2 viral infection and attenuate any COVID-19 disease progression & severity. We identified this connection as early as July 2020 and expanded upon it in October 2020.
The irony increases to epic proportion when you recall that instead of telling a population to get outside, the UK government told everyone to stay indoors. This prevented vitamin D synthesis from UVB exposure, as well as increased viral load. Vitamin D deficiency (<20 ng/ml) was already endemic in the UK and it is no surprise that countries with the highest levels of deficiency have the highest COVID-19 mortality rates.
Public Health England has not only done nothing to prevent this but also made the situation worse by telling us for over a decade that ‘any sunshine=skin cancer, so you better not go outside’. They helped fuel deficiency to epidemic levels, illuminating a landing strip for a virus that is effectively ‘allergic’ to the presence of vitamin D but thrives in its absence.
Leptin Resistance.
Adipose tissue stores body fat before it is converted to energy that the body needs. This metabolic process is overseen by adipokines that are both pro- and anti-inflammatory cytokines. In a healthy person, they are in balance. In an obese person, there is greater expression of inflammatory adipokines, as obesity is a chronic state of low-grade inflammation.
Leptin is the main adipokine. As the cells of the innate immune system express leptin receptors (LEPR), it has a key role in modulating the response to infection. Over time, over-expression of leptin in obese individuals de-sensitises the LEPR, causing a dysfunctional immune response, especially in the early stages of infection. This includes reduced production of IL-1β, IL-6, IL-12 & IFNγ cytokines as well as nitric oxide (𝘵𝘩𝘦 most effective killer of SARS-CoV-2 virions).
SARS-CoV-2 inhibits interferon (IFN) production – through reduced detection by RIG-1, IFIT-1 and MDA5 – so leptin’s role in stimulating IFN is even more crucial.
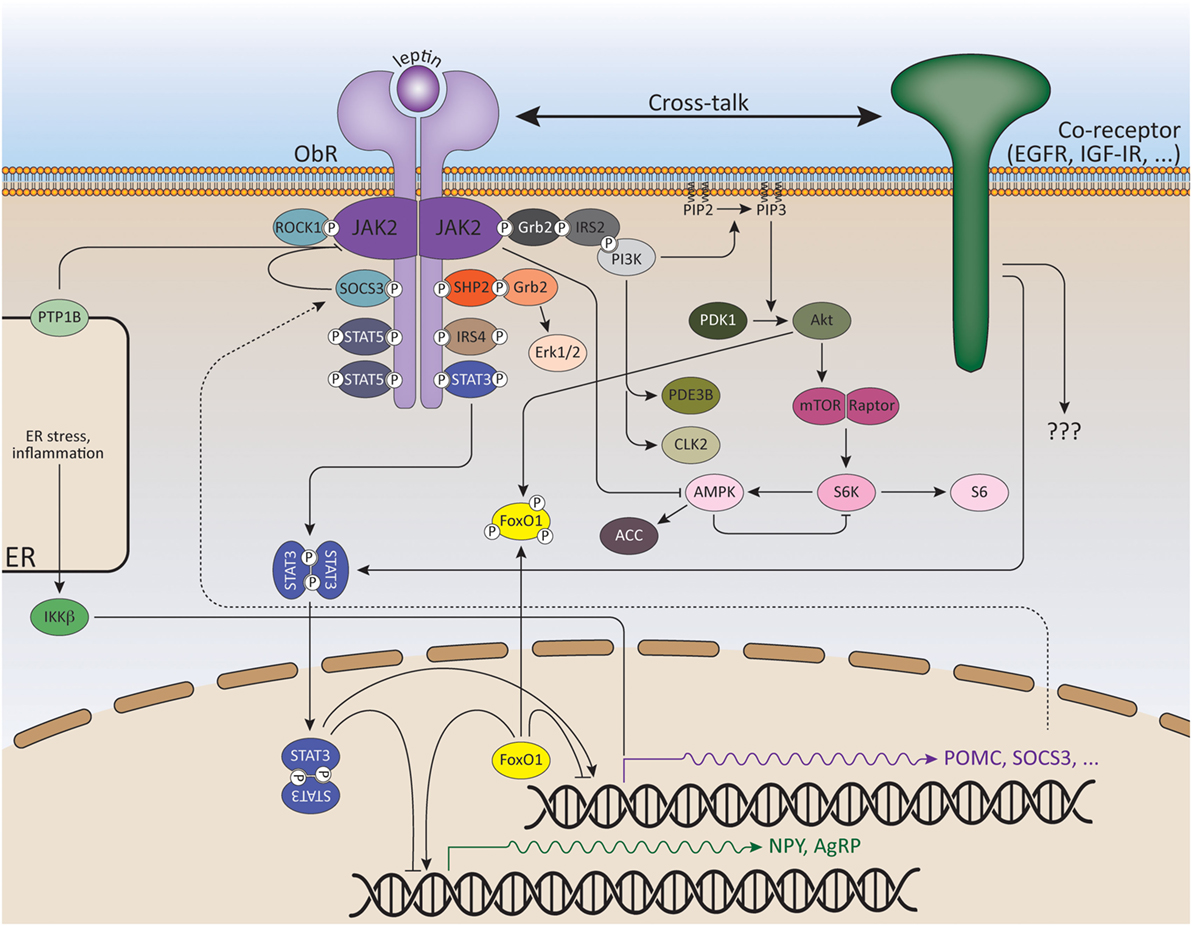
Leptin receptor signalling; Wauman, Zabeau and Tavernier, 2017.
Leptin is also a key requirement in natural killer (NK) cells. While lymphoctyes, NK cells are part of the innate immune response and can naturally recognise antigen, without having to be primed or coded on an antigen-specific basis.
They are effective within minutes of infection, both killing infected cells (by insertion of toxic granzymes) and signalling to other cells (through stimulation of interferon-gamma [IFNγ]). NK cells can help overcome an infection and if not then contain it, allowing time for activation of an adaptive immune response.
Immediate stimulation of NK cells with leptin increases their cytotoxicity, rate of proliferation and IFNγ signalling. Sustained over-exposure to leptin, caused by obesity, de-sensitises NK cells and creates leptin-resistance: this causes decreased NK proliferation, cytotoxicity & signalling as well as increased death of NK cells. This has been known about for years as the below extract from a 2005 study – one of the most authoritative works on the subject – summarises:
“𝘈𝘤𝘲𝘶𝘪𝘳𝘦𝘥 𝘭𝘦𝘱𝘵𝘪𝘯 𝘳𝘦𝘴𝘪𝘴𝘵𝘢𝘯𝘤𝘦, 𝘪𝘯 𝘤𝘰𝘯𝘵𝘳𝘢𝘴𝘵, 𝘮𝘢𝘺 𝘣𝘦 𝘰𝘯𝘦 𝘰𝘧 𝘞𝘦𝘴𝘵𝘦𝘳𝘯 𝘮𝘢𝘯’𝘴 𝘮𝘰𝘴𝘵 𝘱𝘳𝘦𝘷𝘢𝘭𝘦𝘯𝘵 𝘤𝘰𝘯𝘥𝘪𝘵𝘪𝘰𝘯𝘴. 𝘝𝘪𝘳𝘵𝘶𝘢𝘭𝘭𝘺 𝘢𝘭𝘭 𝘰𝘣𝘦𝘴𝘦 𝘪𝘯𝘥𝘪𝘷𝘪𝘥𝘶𝘢𝘭𝘴 𝘢𝘳𝘦 𝘳𝘦𝘴𝘪𝘴𝘵𝘢𝘯𝘵 𝘵𝘰 𝘢𝘤𝘵𝘪𝘰𝘯𝘴 𝘰𝘧 𝘵𝘩𝘪𝘴 𝘷𝘦𝘳𝘴𝘢𝘵𝘪𝘭𝘦 𝘩𝘰𝘳𝘮𝘰𝘯𝘦.” Hyperleptinemia, Unger, 2005.
Public Health England has done nothing to address this increasing risk, instead it has allowed it to become endemic within the population of whose health it is supposed to be overseeing.
Omega-6 Fatty Acid.
Excess omega-6 (n-6) fatty acids produce excess prostaglandin E2 (PGE2). PGE2 is expressed in multiple types of cell throughout the body and it has numerous beneficial functions.
Two of its functions are to stimulate inflammatory IL-17 in the innate immune response to infection and to regulate that ensuing response. PGE2 does the latter by a) suppressing NK cells (see above) both in their cytotoxicity and production of IFNγ and b) disrupting phagocytosis in neutrophils (the most common cell in the innate immune system) and alveolar macrophages. The latter are crucial as they line the lungs and are a binding target for SARS-CoV-2 𝘪𝘧 it reaches the lower respiratory tract, i.e. ground zero for COVID-19 disease severity.
PGE2 also regulates naïve B and T cells, with excess PGE2 stimulating excess apoptosis of healthy cells that would otherwise mature and proliferate as antigen-specific cells within the adaptive immune response. The sustained production of excess PGE2 through excess fatty acid disrupts the immune system in both its innate and adaptive responses
Linoleic acid (LA) is an n-6 that oxidises to 4-hydroxy-2-nonenal (4-HNE). 4-HNE inhibits dimethyarginine dimethylamine hydrolase (DDAH). DDAH inhibits asymmetric dimethyl arginine (ADMA). ADMA inactivates endothelial nitric oxide synthase (eNOS).
eNOS is part of the vitamin D→eNOS→nitric oxide pathway. Nitric oxide is 𝘵𝘩𝘦 most effective killer of SARS-CoV-2, destroying it before it replicates in infected cells. eNOS is therefore essential to provide effective protection and immunity against SARS-CoV-2.
eNOS is inactivated by ADMA but DDAH inhibits ADMA, so DDAH is your friend. 4-HNE inhibits DDAH so is not your friend. 4-HNE is produced from LA.
Daily, fast food deliveries of n-6 laden, COVID-magnet stodge are far more dangerous than SARS-CoV-2. Why they make up every other advert on TV is beyond comprehension and is yet another epic fail from Public Health England, as it promotes a sedentary, indoor lifestyle.
Disrupting The Omega-6:Omega-3 Balance Increases COVID-19 Disease Severity.
Very simply, n-6 is pro-inflammatory and n-3 is anti-inflammatory. Somewhere between our evolution as gnathostomes approx. 500 million years ago and as homo habilis approx. 2 million years ago, we lost the ability to synthesise essential n-6 and n-3 fatty acids, meaning they must be derived from diet. Humans started out with a n-6:n-3 ratio of 1:1 and a ratio of up to 4:1 is considered acceptable.
Since the 1970s, the accelerating rise in consumption of n-6 rich foods – notably refined sugars and high fructose corn syrup – has led to a widening of the ratio: a ratio that is fundamental to health and the function of the immune system. At the same time, there has been a decrease in consumption of n-3 rich foods, stretching the ratio further. The ratio in Western diet now sits around 15:1 to 20:1 and in North America is as high as 25:1. Now you know why 48.4% of COVID-19 total deaths worldwide are in North & South America.
Excessive n-6 leads to a myriad of health problems, with the two main ones being a chronic pro-inflammatory state (diet-induced obesity) and atherosclerosis (hypertension). Obesity and hypertension are the two biggest COVID-19 comorbidities.
Conclusions.
- Lifestyle and diet-induced obesity inhibit key functions of the early stage of the immune response, thereby facilitating SARS-CoV-2 viral infection and COVID-19 disease progression.
- Excessive n-6 is a magnet for COVID-19 disease severity. Eat less n-6, eat more n-3. A simple message that has bypassed Public Health England for years.
- Public Health England has failed completely in its role of ensuring the nation’s health. It has ensured that the UK’s COVID-19 mortality rate is amongst the highest on the planet on a population-adjusted basis and is several times higher than the worldwide average.
- Excess n-6 intake from Western diet weakens one of your key & most effective SARS-CoV-2 defences.
- Obesity is asking your immune system to fight SARS-CoV-2 with one hand tied behind its back.