Background.
It is impossible to ignore the pivotal role of vitamin D both in preventing SARS-CoV-2 viral infection (through the eNOS→nitric oxide pathway) and in reducing COVID-19 disease severity (through the cholecalciferol→ calcifediol→calcitriol pathway). As early as July 2020 we had identified the positive correlation between COVID-19 mortality rate and vitamin D deficiency. By October 2020 we had shown that SARS-CoV-2’s Achilles heel is its vulnerability to nitric oxide within the innate immune response. Nitric oxide in the epithelium is attacking virions within minutes of detection of infection.
Crucially, this innnate immune response is in the upper respiratory tract and is effective against apical ciliated epithelial cells, i.e. the principal target cell to which SARS-CoV-2 binds and fuses. Once again, you do not target a pathogen that binds and replicates in epithelial tissue with an antiviral (they are not vaccines) that is active in endothelial tissue. At the end of week one of the infection cycle, if an individual moves toward COVID-19 disease progression (in less than 0.5% of all those infected unless you follow government advice that causes high viral load in the early stage of infection) rather than toward viral clearance (in more than 99.5% of all those infected), then an antiviral can attenuate the resultant disease progression and severity. This is exactly what an antiviral is designed to achieve (you can read the difference between an antiviral and a vaccine here), with its main objectives usually being to reduce potential hospitalisation and shorten recovery times. With IgG seroconversion taking 6-8 days from initial infection then it is aligned with that end-point of week one. Remember that SARS-CoV-2’s replication cycle takes a little over 10 hours which is why none of the antivirals can prevent viral infection or transmission.
Vitamin D’s Role In Preventing Viral Infection.
Having undertaken further work in January 2021 on nitric oxide, we showed that in addition to its normal universal function against any pathogen, it is also particularly effective against pathogens containing cysteine proteases. SARS-CoV-2’s main protease, 3-chymotrypsin-like protease (3CLPro or Mpro) is a cysteine protease and nitric oxide disrupts its ability to unpack polyproteins pp1a/ab, to cleave the nsps and – most importantly – to oversee the assembly of the RTC. Nitric oxide also targets two of the nsps themselves, nsp3 & nsp4 [Xu et al., 2020]. It also triggers palmitoylation in the SARS-CoV-2 receptor binding domain, reducing the S2 subunit’s binding affinity to the membrane of the host cell.
Vitamin D’s Role In Reducing Disease Severity.
In February 2021, our work on the role of calcifediol in attenuating COVID-19 disease progression and severity was validated by Nogués et al.‘s study that shows administering high dosage calcifediol to those hospitalised with COVID-19 disease severity reduces disease progression by 74% and mortality by 57%. Quite staggering results simply from high levels of vitamin D.
Initially it was puzzling and now it is incredulous that these key roles of vitamin D both in preventing SARS-CoV-2 viral infection and in attenuating COVID-19 disease severity have been ignored by Public Health England and the NHS. These organisations continue not just to ignore the fact but also to dismiss it, pilloring those who point out that vitamin D plays a central role. Vitamin D regulates nitric oxide production and has been doing so since humans first evolved. To pretend that it doesn’t work for SARS-CoV-2 is insane and absurd. Is it any wonder that the UK’s COVID-19 mortality rate is 3.2-times higher than the worldwide average?
Vitamin D attenuates disease progression. It saves lives. Had the NHS listened to fact and not ignored it in favour of its own deadly arrogance and propaganda, over 75,000 UK deaths would have been avoided.
TLR2 Signalling Pathway.
Some of our most recent work suggests that Public Health England and NHS need still more reminding of the role played by vitamin D in enabling a strong innate immune response. Remember, SARS-CoV-2 is all about viral load in the upper respiratory tract and a robust innate immune response counters the risk factor of high viral load, especially in the early stage of infection.
Epithelial cells in both upper & lower respiratory tracts express pattern recognition receptor TLR2. As previously explained, TLR7; TLR8 and on a good day TLR3 detect viral pathogens, including SARS-CoV-2. The relevance of TLR2 is that is is highly expressed in epithelial tissue and so is present in the upper respiratory tract. Upon detection of antigen, TLR2 begins a signalling pathway;
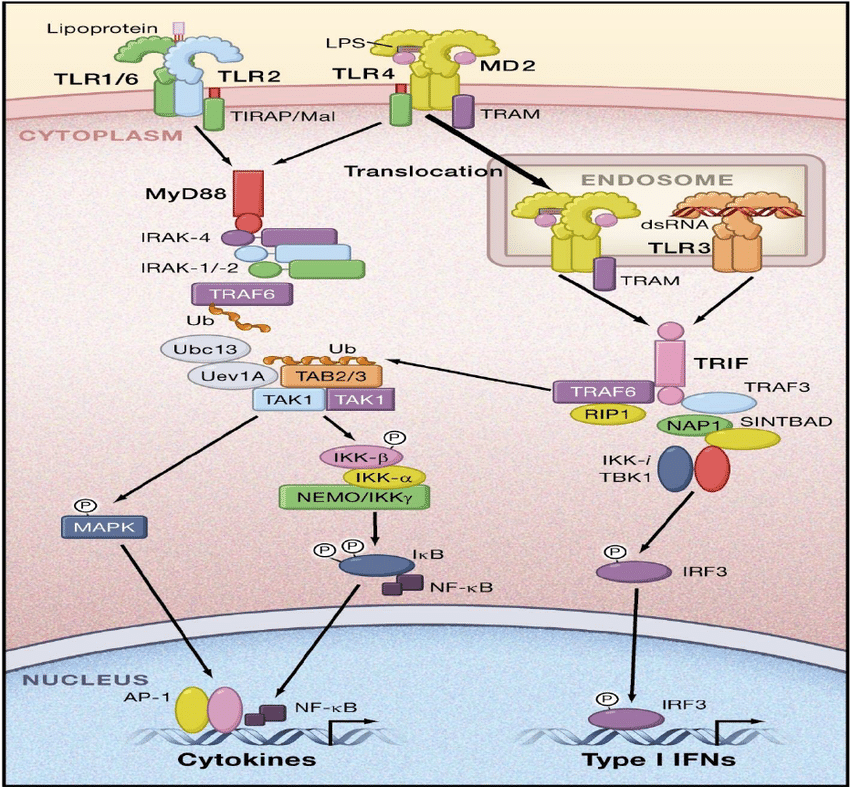
TLR signalling pathway, source: Researchgate.
Cathelicidin Antimicrobial Peptide.
This includes activation of the vitamin D receptor and its hydroxylase, allowing it to bind calcitriol (active vitamin D) forming a VDR:D3 complex, which upregulates cathelicidin (in full, cathelicidin antimicrobial peptide or CAMP). CAMP is expressed across the main cells that form the innate response, as well as in the very apical epithelial cells to which SARS-CoV-2 fuses.
CAMP assists with the phagocytosis of infected cells and as it is induced by TLR2, it performs a key role in the early stage of the innate immune response.
Pattern recognition receptors can be thought of as ‘radar stations’ that are constantly searching for ‘non-self’. As TLR7 and TLR8 are endosomal they can only detect antigen once it has entered the intracellular space, i.e. after binding and intracellular fusion. TLR2 is located on the cellular membrane meaning that it is, in effect, an earlier warning radar station than TLR7 and TLR8. This allows for earlier activation of the innate immune response.
TLR2 is located at ground zero for SARS-CoV-2 viral infection, detecting antigen, recognising it and giving the green light for vitamin D activation to produce CAMP. Do you think that it does this more effectively with a healthy or low level of vitamin D?
Vitamin D deficiency inhibits the production of CAMP and inhibits the innate immune response to SARS-CoV-2. This should not be beyond the understanding of those supposedly in charge.